1601006012 long case
A 55 year old female from nakrekal, a daily wage labourer, a known case of CKD presented to the opd with chief complaints of
- Fever since 5 days.
- Loss of appetite since 5 days.
- Difficulty in breathing since 5 days.
- Reduced urine output since 2 day.
History of presenting illness :
- Patient was apparently asymptomatic 15 days back when she developed cough with mucopurulent greenish yellow expectoration, increased at night, no relieving factors.
- Fever - Since 5 days, Low grade, insidious in onset, associated with chills. There was evening rise of temperature. It was relieved on medication.
- Shortness of breath - Since 5 days, Grade 2, Increased on exertion, talking, eating. Reduced on taking rest. Not associated with orthopnea or nocturnal dyspnea.
- Reduced urine output since 1 day associated with abdominal distension and pain.
No history of chest pain.
No history of Diabetes, Hypertension, Asthma, Epilepsy, Tuberculosis.
Past history :
No similar complaints in the past
Medical history :
Not significant
Family history :
Not significant
Personal history :
Sleep - adequate
Bladder - reduced urine output
Bowel - regular
Appetite- reduced
Diet - mixed
Addictions -
Smoked chutta 1/day for 40 years
Chronic alcoholic since 40 years
GENERAL EXAMINATION
Patient is conscious, coherent, coperative ; moderately built and moderately nourished.
No pallor, icterus, clubbing, edema, koilonychia or lymphadenopathy.
Central line for dialysis present.

Vitals
Temperature: Presently afebrile
BP: 115/70 mmhg
RR:26 cpm
PR:80 bpm
PO2 : 97 mmhg
SYSTEMIC EXAMINATION:
Respiratory system :
Inspection:
Shape of the chest : Normal (Transverse diameter(27cm) > AP(23cm))
Symmetry of chest : Symmetrical
Respiratory movements : Equal on both sides
https://drive.google.com/file/d/1dIcFF7-VBw200vCq5eAR1hjCYNxLAha1/view?usp=drivesdk
Trial sign : Negative
Dilated viens : Not present
Deformities of spine : Absent
Apical impulse : cannot be seen
Scars : None on the chest
Pulsations : Absent
Palpation :
(Inspectory findings are confirmed)
Tenderness: Absent
Chest circumference :74.5 cm on full inspiration

Expansion equal on both sides - Anterior and posterior.
Trachea: not deviated
Apex beat: 5th Intercoastal space
Vocal fremitus felt equally in all areas
Percussion :
Direct percussion over the clavicle was resonant on both sides.
Indirect percussion
Anterior:
Supramammary - resonant on both sides
Inframammary - resonant on both sides
Posterior:
Suprascapular - resonant on both sides
Interscapular - resonant on both sides
Infrascapular - dull in the right and resonant in the left (persistent dullness on tidal percussion)
No shifting dullness observed.
https://drive.google.com/file/d/1PzN1igJqb2544QHuPyBcLUDQe3qSDHAC/view?usp=drivesdk
Auscultation:
Bilateral air entry present.
Normal vesicular breath sounds heard in supramammary, Inframammary, suprascapular area of both sides.
Reduced breath sounds in infrascapular and infraaxillary area of right lung.
No added sounds
CVS examination :
S1 and S2 heard
No murmurs
No palpable thrills
Abdominal examination :
Scaphoid shape
No tenderness
No palpable mass
No organomegaly
No ascites
Bowel sounds present
CNS examination:
Conscious and alert
Normal gait
Normal speech
No focal neurological signs
All reflexes are intact
Fever chart :


INVESTIGATIONS :
CBP

ABG

CUE

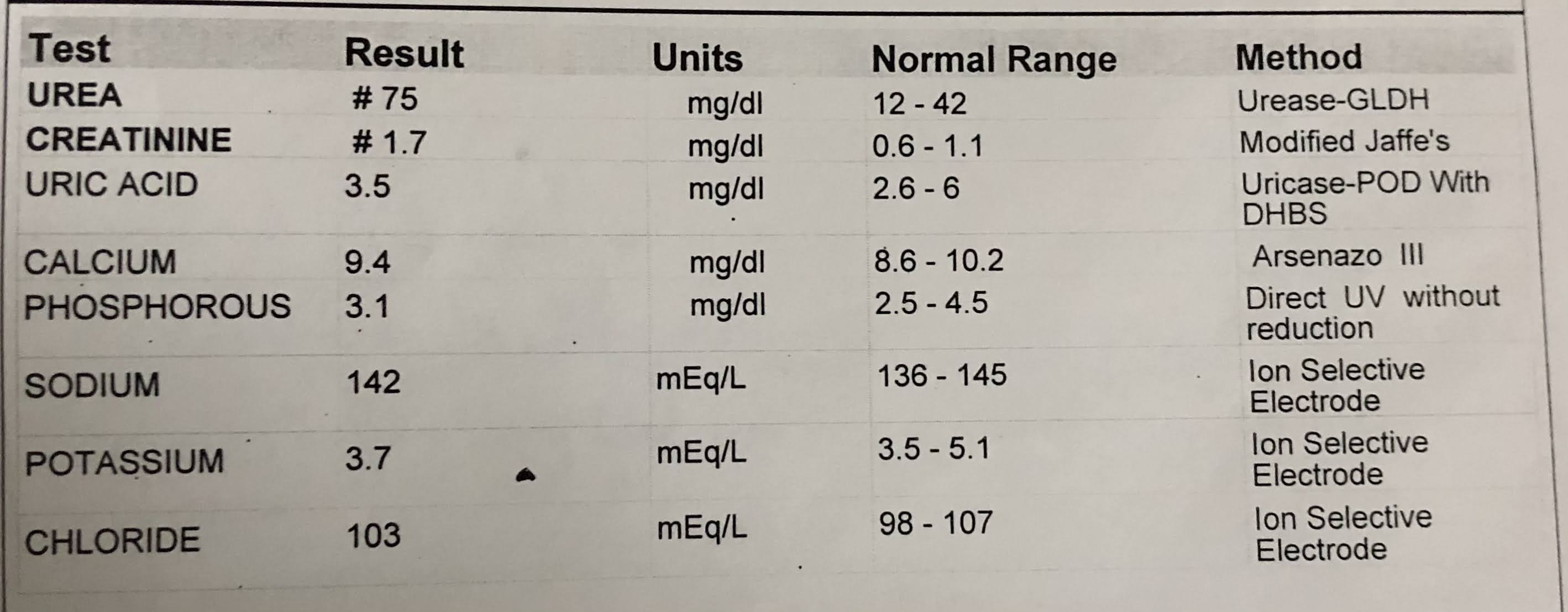
RFT
LFT

PT / APTT - 15 secs / 30 secs (normal)
Blood sugar - 207 mg/dl (fasting) - high
RTPCR - Tb - Negative
Widal - No agglutination
Dengue NS1 - negative
Serum creatinine - 7.6 mg/dl

ESR - 70 mm (raised)
Serum potassium - 4.9 (normal)
Blood culture - Ecoli isolated which was sensitive to cotrimoxazole and meropenem.
Chest xray :

Cardiac size is normal. No mediastinal abnormality.
Bilateral lung fields show multiple microcalcific regions. (Can be secondary to age)
Peripheral pulmonary vasculature is normal.
Domes of diaphragm shows smooth outline at normal positions.
Bilateral hila are normal in size and have equal density, bear normal relationship.
Bilateral pleural spaces are normal.
Visualised bones and soft tissues are normal
No abnormality detected.
ECG - normal

HRCT :
Suspicious ground glass opacity noted in left lower lung field - CORADS 3
Bilateral minimal pleural effusion. Loculated effusion on right.
Basal atelectasis noted involving left lower lung fields.
Left staghorn renal calculus.
Visualised portion of bones appear normal.
TREATMENT :
Started on ATT











Comments
Post a Comment